It’s 7:30 AM. You are getting ready for work or college, looking in the mirror, and there it is: a distinct, tender red bump sitting squarely on your cheek. You try to squeeze it, but nothing happens—it just gets redder, angrier, and more swollen.

A few days later, a different kind of guest appears: a blemish with a bright, glaring yellow-white center staring right back at you.
In India, we grow up hearing endless advice for these moments. "Stop eating so much mango," "Apply a dab of toothpaste," or "Just put some haldi (turmeric) on it." But when you try to research how to fix it online, you are hit with confusing slang: pimples, zits, bumps, spots. Are they all the same thing? Yes and no.
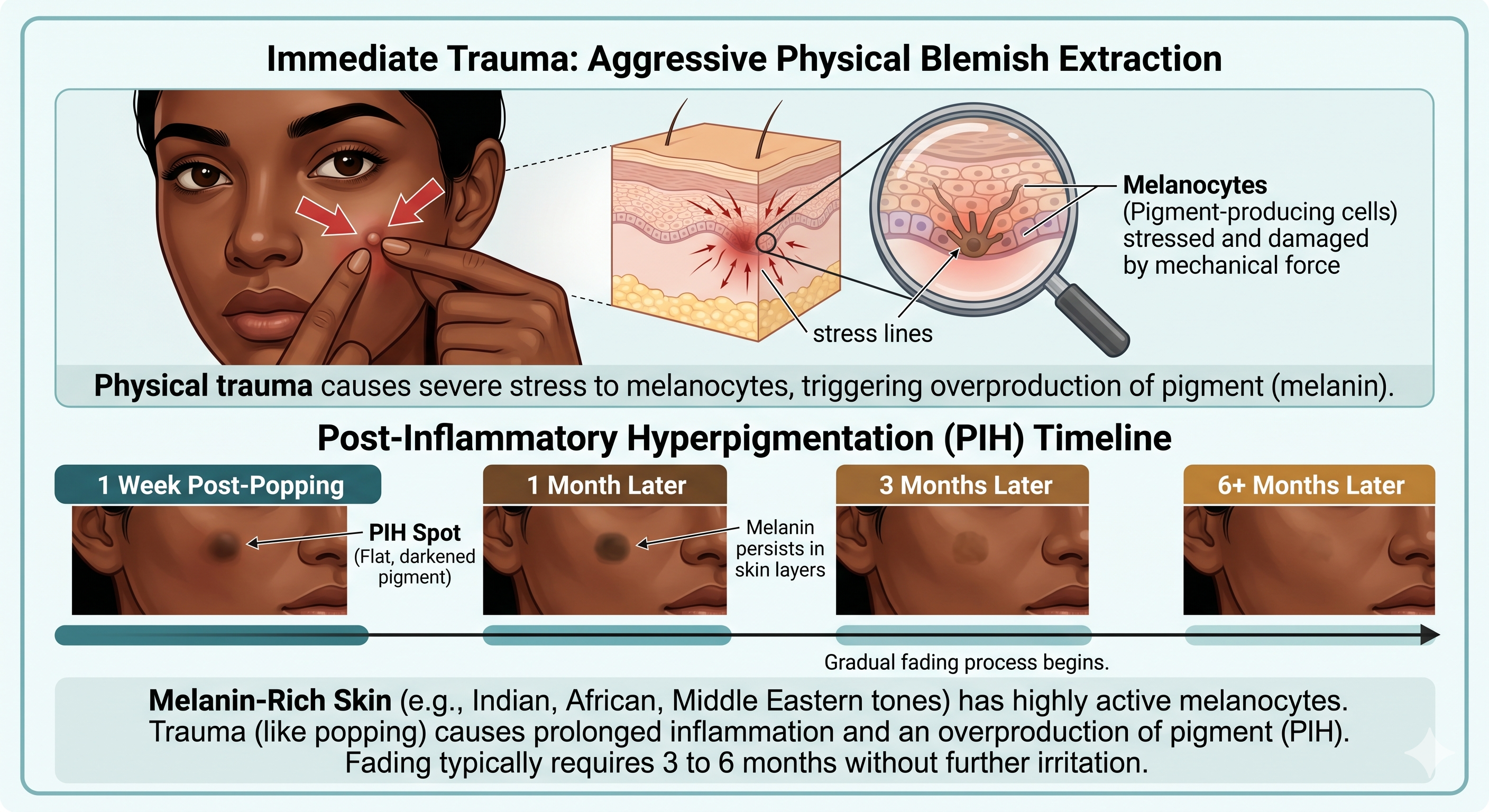
In the world of clinical dermatology, the words "pimple" and "zit" are casual umbrella terms used interchangeably by everyday consumers. However, beneath the surface, your skin is dealing with very specific stages of localized warfare. To treat them without leaving stubborn dark marks (Post-Inflammatory Hyperpigmentation—a massive challenge for melanin-rich Indian skin), you need to know exactly which stage you are looking at: an Inflammatory Papule or an Inflammatory Pustule.
Let’s decode exactly what is happening under your skin.
Every acne blemish starts the exact same way: a microscopic clogged pore (microcomedone) trapped by excess sebum and dead skin cells. But when normal skin bacteria like Cutibacterium acnes feed on this trapped oil, your body's immune system sets off an alarm, triggering an inflammatory response.
Depending on how your immune system fights back, you get one of these two primary inflammatory lesions:
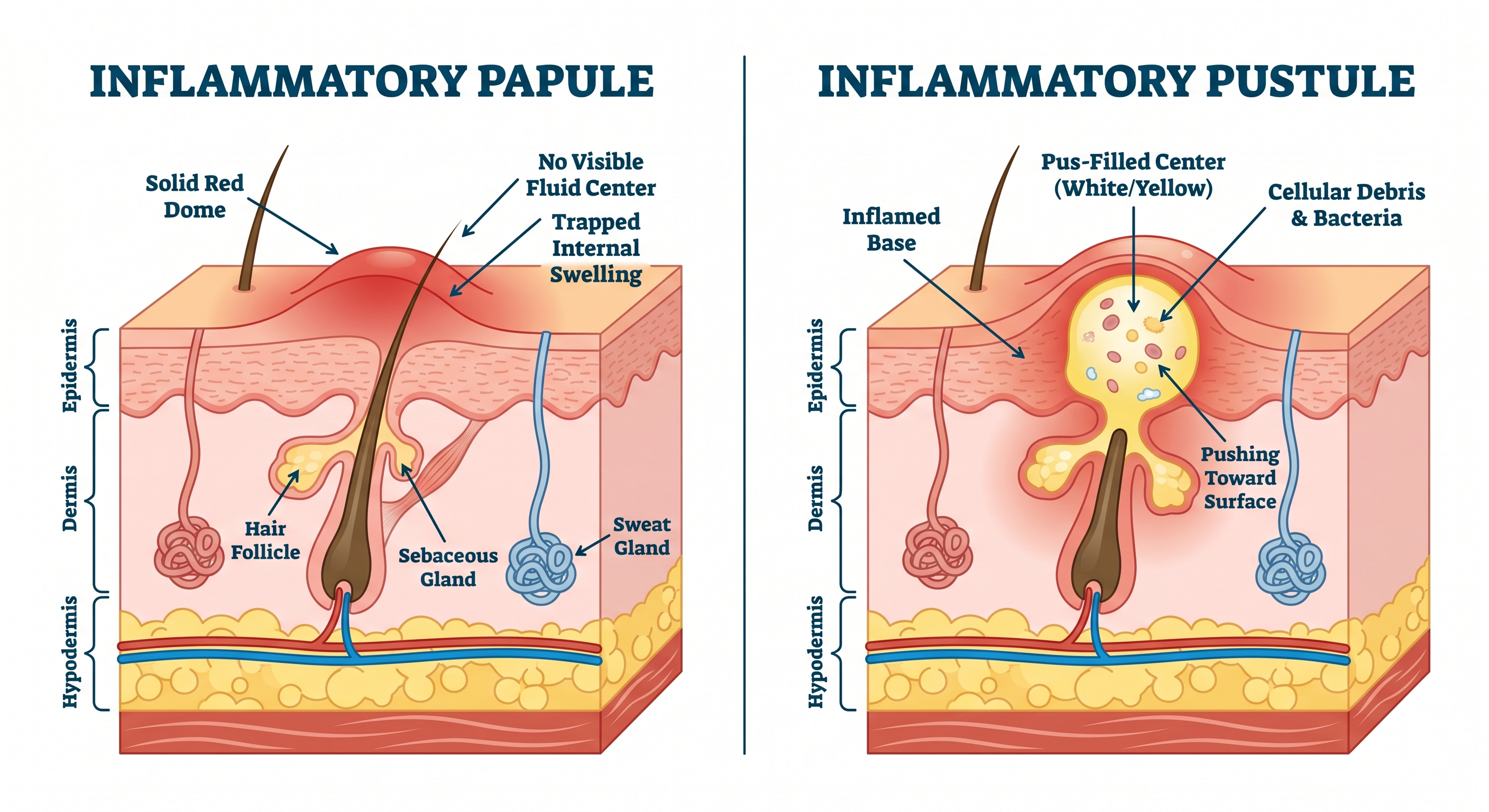
1. The Inflammatory Papule (The "Blind" Red Bump)
What it looks like: A small (usually under 5mm), raised, solid red bump on the skin.
The Defining Trait: No visible pus. It does not have a white or yellow "head".
How it feels: Tender to the touch, tight, and locally inflamed.
What is happening inside: A papule occurs when the cellular wall of your clogged pore breaks down deep within the outer layer of the skin (epidermis). Your body sends white blood cells to surround the infection, causing sudden swelling and visible redness driven by dilated blood capillaries.
2. The Inflammatory Pustule (The Classic "Zit")
What it looks like: A distinct raised bump featuring a red, inflamed base ringed around a highly visible white or yellow center.
The Defining Trait: Packed with pus.
How it feels: Painful, but often feels slightly softer at the absolute tip compared to a hard papule.
What is happening inside: A pustule is essentially a papule that has matured and "come to a head". That yellowish liquid isn't just dirt—it is the direct aftermath of your immune system's battle. It is a collection of dead white blood cells, cellular debris, and bacteria that your body is actively trying to push out to the surface of the skin.
Pimple is the widely accepted layperson term for any small inflammatory skin lesion (papules or pustules).
Zit is purely highly popularized Western slang for a pimple.
However, in everyday usage, people tend to use "pimple" when referring to the early, hard red bumps (papules) and reserve "zit" for the highly poppable, liquid-filled stage (pustules). Understanding this distinction helps you choose the right active skincare ingredients rather than attacking the skin blindly.
| Feature | Inflammatory Papule | Inflammatory Pustule |
|---|---|---|
| Commonly Called | Red Pimple / Blind Bump | Zit / Classic Pimple |
| Visible Fluid Center? | No. Solid red dome. | Yes. White/yellow cap. |
| Primary Contents | Trapped inflammation & swollen tissue. | Pus (dead white blood cells & debris). |
| Poppable? | Absolutely Not. Squeezing pushes bacteria deeper. | Technically yes, but medically discouraged to prevent scarring. |
| Stage | Early-to-mid inflammatory response. | Late-stage localized immune response. |
Hot and humid weather, heavy pollution, and higher natural melanin production make managing breakouts on Indian skin uniquely challenging.
Humid monsoons and summer heat accelerate excess sebum production. This combined with a drop in helpful skin bacteria allows persistent inflammation to take hold more easily. Furthermore, Indian skin is highly prone to Post-Inflammatory Hyperpigmentation (PIH).
To treat these lesions effectively, we must look at clinically backed topical agents rather than relying on harsh localized friction.
How to Treat an Inflammatory Papule (Calm the Fire)
Because a papule has no open pathway to the surface, your goal is to penetrate and soothe, not extract.
- Salicylic Acid (BHA): Being oil-soluble, it dives deep into the sebaceous lining to dissolve the hardened plug causing the backup.
- Topical Retinoids (Adapalene/Tretinoin): Vitamin A derivatives normalize how your skin sheds cells, preventing microcomedones from forming while reducing lingering redness. (Note: Retinoids must be introduced slowly at night to avoid irritating the skin barrier).
- Ice Cycling: Gently applying a wrapped ice pack for 30 seconds can constrict the localized blood vessels, instantly dropping the swelling and throbbing pain.
How to Treat an Inflammatory Pustule (Clear the Debris)
Because the infection sits right at the surface, your goal is bacterial neutralization and safe drainage.
- Benzoyl Peroxide (2.5% to 5%): The gold standard in clinical dermatology. It introduces oxygen into the pore, effectively destroying the anaerobic C. acnes bacteria while drying out the localized pus collection.
- Hydrocolloid Patches (Pimple Patches): A lifesaver for Indian heat. Applying a patch over a ripe pustule absorbs the excess fluid safely overnight while physically blocking your fingers from picking and causing PIH.
Q: Can I use multani mitti (fuller's earth) on active papules and pustules?
A: Proceed with caution. While multani mitti is excellent for absorbing surface sebum in hot Indian summers, letting it dry completely hardens the skin. This can severely strip your natural skin barrier, triggering your oil glands to overcompensate and produce even more sebum, worsening inflammatory lesions. If you use it, rinse it off while it is still semi-wet.
Q: Why do my papules never turn into pustules?
A: Not all papules are destined to come to a head. Sometimes, your body successfully breaks down and reabsorbs the internal inflammation without needing to push cellular debris to the surface. Squeezing a persistent papule will only cause an internal rupture, turning a minor bump into a severe, deep nodule.
Q: When should I see a dermatologist instead of using OTC serums?
A: Seek clinical help if your inflammatory bumps are highly widespread, leave deep pitted scars (atrophic scarring), or do not respond to basic OTC treatments after 6 to 8 weeks. Persistent deep lesions concentrated around the jawline in women may also point toward internal hormonal imbalances like PCOS, requiring targeted internal management beyond surface skincare.